Are You Ready To Consent To A Heart Transplant
Part of the Transplant Work up is for you and your partner/family/carer, to discuss the sobering and humbling statistics of transplant success rates and related risks.

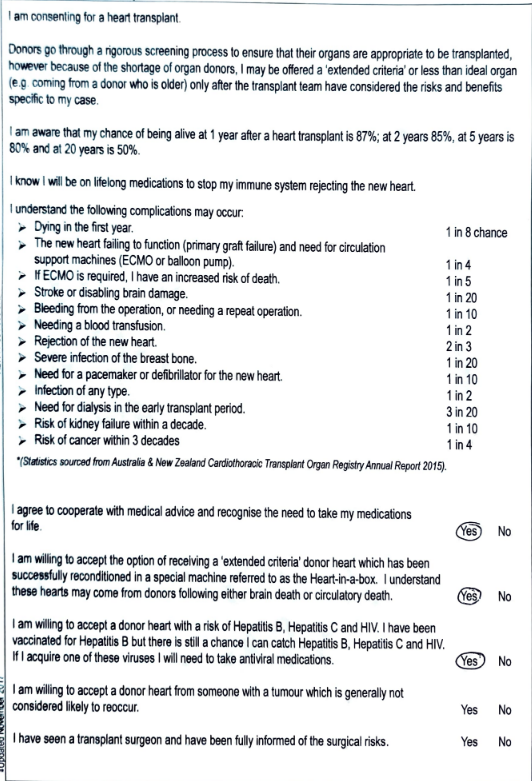
Heart Transplant statistics
Consenting to a heart or lung transplant is a daunting challenge to face. Part of the Transplant Work up is for you and your partner/family/carer, to discuss the sobering and humbling statistics of transplant success rates and related risks. Due to the short timeframe between collecting and transplanting a donor organ, the organ can not be pre-screened for certain conditions and infections. You will need to consider the potential risk for a donor organ to have Hepatitis B, Hepatitis C and or HIV. These illnesses are not considered life threatening and are treatable. They are considered a tolerable risk if you are terminally ill.
Heart transplant waiting list
Early on in the process of the work up for listing, my husband and I were in an office with my specialist and he took a call. We could hear the whole conversation. A transplant team member was informing the specialist that a donor heart had become available. The donor had suffered a drug overdose. They discussed possible recipients based on matching gender, size and weight. They also considered which recipient was less likely to survive without the transplant.
ECMO (Extracorporeal Membrane Oxygenation)
While I was in ICU there was a patient on ECMO after a double lung transplant. ECMO (Extracorporeal Membrane Oxygenation) temporarily takes over the work of the lungs and/or the heart. The machine adds oxygen to the blood and then pumps the oxygen-rich blood back through the body. Be reassured that if you do need ECMO you will be unconscious with a general anaesthetic.
Hepatitis C risk
After my heart transplant I was up in a ward with three other patients. The transplant team came into our ward to tell one of the double lung transplant patients that she had contracted Hepatitis C from the donor organ.
Other Complications
Please see the post on Benefits and Risks of Heart / Lung Transplant to learn more.
Rejection
I have been fortunate not to have the complications discussed above. However, I have been in and out of rejection for the first 4 months post transplant. Each time I was in moderate to severe rejection I was readmitted to St Vincent’s for 3 days for 1000mg IV Prednisone. It takes many weeks to gradually reduce the dose of oral prednisone. Meanwhile you may see increased weight, puffy face, sleeplessness and increased anxiety to name a few side effects. Eventually the team stabilises your medications and hopefully rejection will be a bad distant memory. 10 months on, I have regular Cardiac MRI to monitor for rejection. Please let me know in the comments if you have reoccurring rejection. I have met quite a few Heart Transplant recipients that experience rejection many years after transplant.
Internal Jugular Vein Damage
The CVL, Central Venous Line is placed in an IJV, Internal Jugular Vein which administers medications during and after a transplant or major operation. After my transplant my Right IJV developed a clot which became chronic. Clots are treated with blood thinners via injection and or orally. I used Clexane Injections and then transitioned to oral Warfarin for many months. This eventually lead to the RIJV being completely obliterated or non-patent, all fancy words for fully blocked. This has meant that the External Jugular Vein is now draining 100% of the blood from the Brain’s right side rather than the usual 10 to 20%. If you look at the right side of my neck it looks bruised and purple and the pulse is extremely noticeable. This is from the increased blood flow. I can no longer have CVL in left or right IJV as the right is non patent and the left IJV must be protected at all costs.
Please leave a comment if you have a brief story to share or a message of hope to recipients and future recipients.
X
Wednesday
My Consent Form